Telemedicine App Development in 2026: Cost, Features, and Timeline

The shift toward virtual care that began during the Covid-19 pandemic has changed many corners of health care, and few of them as lastingly as the way patients now expect to see a doctor. What started as a temporary substitute for the in-person visit has settled into a permanent habit, and that durability is precisely what makes telemedicine such a compelling place to build in 2026. According to Fortune Business Insights, the global telemedicine market was valued at roughly $113 billion in 2025 and is projected to grow to about $123 billion in 2026 on its way to $441 billion by 2034, expanding at a compound annual rate of more than 17%. While numbers of that scale point to an enormous opportunity, they also signal how much remains to be built before telemedicine becomes a truly stable fixture of modern care.
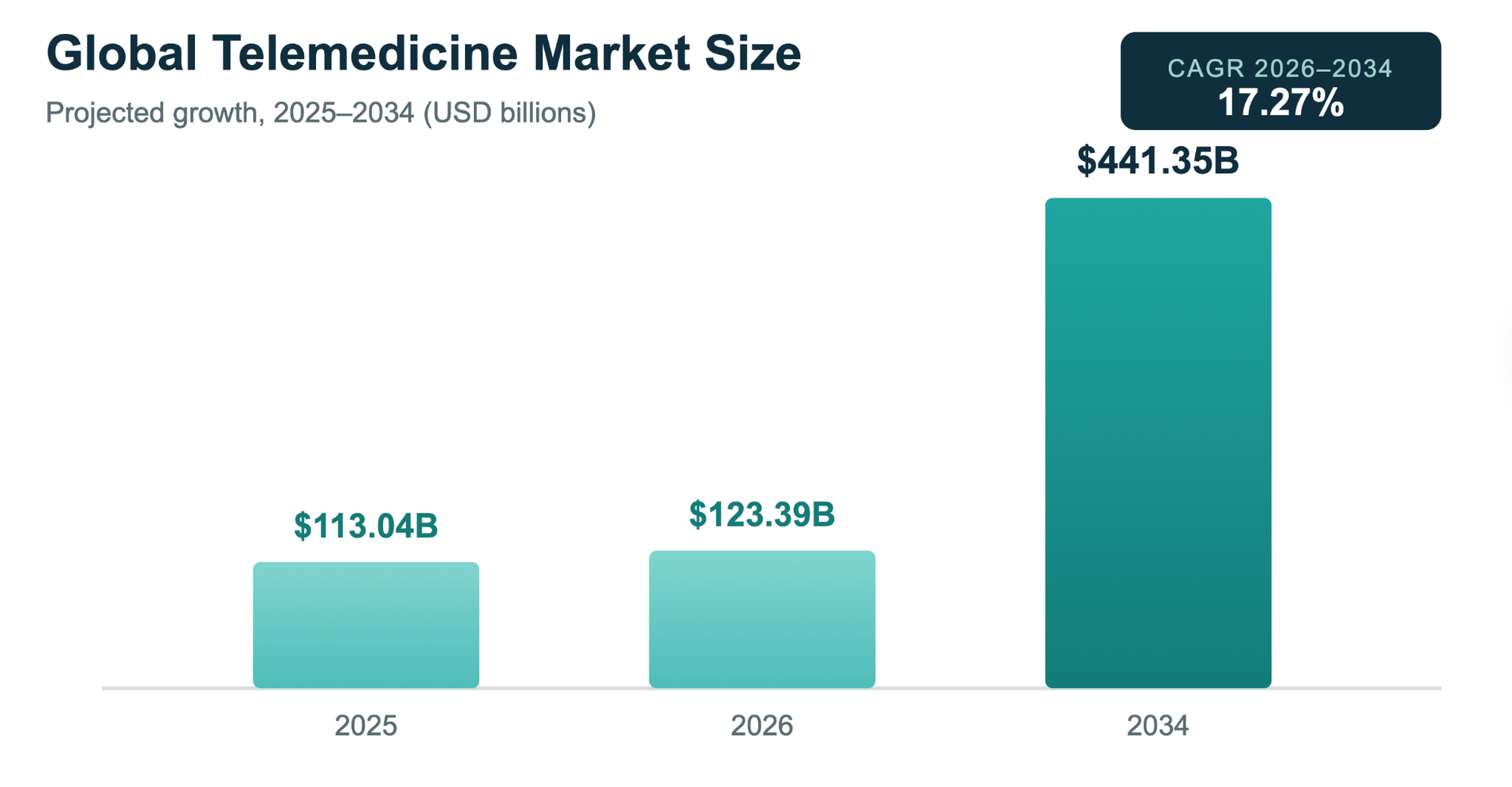
Source: Fortune Business Insights, Telemedicine Market Report
That distinction matters for anyone weighing a build, because the appetite for virtual care has been proven, while the quality of the software serving it still varies widely. The more recent data only reinforces the point, since FAIR Health's claims tracking showed that roughly 18% of insured patients were still filing telehealth claims in early 2026, a habit that has held steady well after the original urgency faded. When demand persists without a crisis pushing it, the real question is no longer whether to build a telemedicine app, but how to build one that genuinely earns its place.
Designing For The Patient Who Comes Back
It is tempting to think of a telemedicine app as little more than a video call wrapped around a login screen, yet the video call has become the part patients take for granted rather than the part that keeps them. The lasting value, as usage patterns make clear, lies in the care that continues over time rather than in the single appointment that ends and is forgotten.
This is borne out in how people actually use these platforms, since mental health care alone accounted for more than half of telehealth patients in early 2026, and that kind of care is rarely a one-time visit. It unfolds gradually, through recurring sessions and ongoing follow-ups, which means the product that succeeds is the one built to carry a relationship rather than simply host a conversation.
Holding onto that idea makes the harder questions of features, cost, and timeline far easier to answer, because each of them flows from the same decision. Once you accept that you are building for everything that happens between appointments, the product's priorities begin to take shape.
The Features That Earn Their Keep
Every credible telemedicine product rests on a familiar foundation that serves both sides of the screen: patients need simple sign-up, scheduling, secure video, messaging, and a way to pay, while providers need a clean dashboard, documentation tools, and a calendar that fits the rhythm of the practice. None of this is glamorous, and yet it is precisely this groundwork that turns a promising demo into something a clinic will trust to run its day.
The return on getting it right can be measured plainly, since telehealth tools have been shown to reduce no-show rates by roughly half, and because a missed appointment represents both lost revenue and a gap in someone's care, cutting that number does real good in two directions at once. For many practices, this single improvement is enough to justify the entire investment.
The feature that quietly determines whether a health system will take a product seriously, however, is the one patients never see: how the app communicates with the hospital's existing record system. Connecting to platforms such as Epic or Cerner is what allows a patient's history to travel with them rather than becoming stranded in yet another silo, and the standard that makes this possible is HL7 FHIR, now the common language through which clinical data moves between systems. The engineers at ScienceSoft frame this kind of EHR-connected telemedicine as the path to genuine care continuity rather than a checkbox, and that framing is the right one, because an app that cannot place a visit note where the next clinician will look for it has made care more convenient without making it any better.
What It Actually Costs
Most people arrive at this question hoping for a single figure, and the honest answer is that none exists, since no two telemedicine apps are truly the same product. A simple browser-based platform, by Cleveroad's estimate, requires somewhere between 600 and 900 hours of work, which translates to roughly $24,000 to $54,000, though that approachable starting point tends to understate how much a serious clinical product asks for beyond it.
The figures rise steadily with ambition, as a production-ready app on a single platform generally lands closer to $100,000 to $175,000; a full build across platforms reaches $150,000 to $300,000 or more, and once deep EHR integration enters the picture, ScienceSoft places the range at $150,000 to $400,000. The breadth of that spread is not vendors hedging their bets but rather an honest reflection of how much the software is being asked to carry.
Two costs in particular deserve to be named early, since both are far cheaper to plan for than to repair after the fact. The first is HIPAA compliance, which is not a box to be checked at the end but a layer woven through the entire build, and skipping it early does not so much save the expense as defer it to a more painful moment later. The second is EHR integration, which carries its own certification and ongoing upkeep for every system connected, so that the cost grows quietly with each one added, and a quote that omits either of these is not the cheaper option but simply the unfinished one.
How Long Does It Take
Time tends to follow money here for much the same reasons, since a focused first version can move quickly, with an MVP often built in two to four months, while a mid-tier product usually takes five to nine months, and a full enterprise platform runs well beyond that as integrations and compliance work accumulate.
What stretches a schedule is almost never the writing of code but rather the waiting that surrounds it, whether for compliance reviews, EHR certifications, or the outside parties who keep their own pace. The teams that manage to stay on track are usually those that invest a few weeks at the very start in mapping precisely what compliance and integration will demand, before those decisions harden into something expensive to undo.
The Question Beneath Every Other One
Underneath all of these considerations sits one quiet question that ultimately settles the rest: whether the care being delivered will actually be reimbursed. That single question is what turns policy from a footnote into a central line in any business plan.
The American Medical Association is currently backing the CONNECT for Health Act of 2025, which would permanently lift Medicare's geographic restrictions and remove the in-person requirement that precedes telemental health visits, and the fact that only a small share of eligible Medicare spending was actually billed as telehealth in 2024 reads less like a ceiling than like considerable room left to grow. The caution worth keeping in view is that much of today's framework still rests on waivers Congress has chosen to renew rather than make permanent, and any honest plan should account for that uncertainty rather than tuck it quietly out of sight.
The Bottom Line
Telemedicine app development in 2026 is no longer about catching a trend, since the market has clearly shown it intends to stay. The teams that come out ahead are usually the ones that treated compliance and interoperability as the groundwork. And the cost is real, ranging anywhere from a modest MVP to a platform worth several hundred thousand dollars, yet the demand waiting on the other side of that work continues to grow, and now is a good time for anyone serious about this space to look closely at their roadmap and plan the build properly.



